
 A medical study [pdf link] has just been published that looks at hospital emergency department (ED) visits for concussions (or to use the clinical term, traumatic brain injuries or TBIs) to children arising from playground incidents in the USA.
A medical study [pdf link] has just been published that looks at hospital emergency department (ED) visits for concussions (or to use the clinical term, traumatic brain injuries or TBIs) to children arising from playground incidents in the USA.
My aim in this post is to give a summary of the study and to scrutinize some of its conclusions. I plan in a future post to discuss its wider implications.
The study used data from a national injury surveillance system to work out injury rates for each year between 2001 and 2013. It also looked at whether or not children were admitted to hospital and the playground equipment involved, amongst other factors, and it analysed the data for trends. It claims to be the first national study on playground-related TBIs since 1999.
The study is important not only because of its new data, but also because it has led to widespread media coverage in the USA. Moreover, it has been widely discussed within the playground safety community. I understand that it has been circulated to members of one of ASTM’s playground safety committees by the Centers for Disease Control and Prevention. Members tell me that it is being seen by some as providing evidence for reviving the playground surfacing proposal that ASTM ultimately rejected last year.
I would welcome comments on the summary offered below, and on what the findings might mean: both for playground safety, and for children’s health and development.
What did the study find?
The study found an average of around 35 ED visits per 100,000 children under the age of 14 per year over the 13-year period. The figure was higher for children aged 5 – 9 years (53.5 per 100,000 per year).
The study found that on average, 2.6% of the children visiting ED were admitted to hospital: a rate of 0.9 children per 100,000 per year. This suggests that the vast majority of playground-related TBIs would – to quote the paper – “likely be best categorised as mild in severity.” (Clinicians typically categorise TBIs as either mild, moderate or severe, depending on the presenting symptoms.)
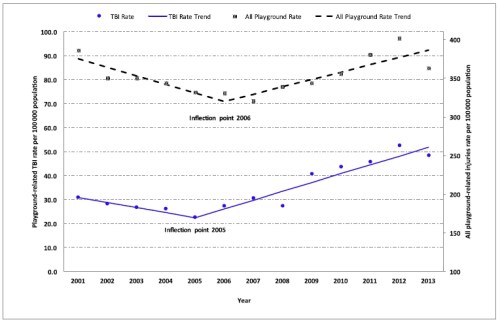
The study also found that visits had increased over the period (a finding picked up by much of the media coverage). However, the increase was not constant. It found a slight decrease over the years 2001-2005, followed by a more significant increase for 2006-2013. Much of the media coverage did not discuss this pattern, but focused on the rise. The average rate rose from around 22/100,000 in 2005 to around 50/100,000 in 2013.
The study also looked at ED visits in relation to different types of playground equipment. It found that monkey bars/playground gyms accounted for 28% of visits, with the same percentage for swings. Slides accounted for 18% of visits. However as the paper notes, it is not possible to draw conclusions about relative risk from this study, because of the lack of data on children’s usage of different types of equipment.
In lay terms, what do the figures mean?
The figures show that an average American elementary (primary) school of 500 pupils would expect to see around one ED visit from a playground-related TBI every 5 or 6 years. As already noted, the figures for hospitalization were much lower. They mean that a city with a total population of around 700,000 – about the size of Memphis, Tennessee – would expect to see one hospital admission each year due to a playground-related TBI.
What are TBIs?
Traumatic brain injuries are injuries to the head that give rise to clinically defined symptoms such as loss of consciousness, and that are caused by external factors (rather than by existing medical conditions or illnesses). They are typically a result of impacts with other objects or the ground. The word ‘traumatic’ is used in the medical sense, to describe an injury caused by an extrinsic agent. The clinical term does not imply any long-term consequences. This is in contrast with ordinary usage, where the word ‘traumatic’ does imply longer-term problems.
What happened to the injured children?
Apart from looking at whether or not they were admitted, the study itself did not follow up what happened to the injured children. However, other studies show that TBIs can have serious and life-changing consequences, including physical impairments, lowered cognitive skills, and behavioural problems. The consequences vary depending on the severity of the injury. As already noted, this study suggests that the vast majority of playground-related TBIs are mild.
What are the health implications of mild TBIs?
The paper states that “TBIs, even those categorised as ‘mild’ can have serious implications”. The study itself does not provide new evidence for this (as already noted, there was no follow-up data). The paper cites four other papers in support. However, this supporting evidence is not strong. Two of the studies cited do not look at mild TBIs, so they cannot support this claim. A third study found a strong association between severity of TBI and outcome (the more severe the TBI, the worse the outcome). The final study cited did find evidence of adverse outcomes for mild TBIs. However, the study’s authors note that this may have been because of pre-existing conditions and not a result of the TBI itself (the study design ruled out claims about cause and effect).
I plan to return in a future post to this important question about the implications of mild TBIs.
How do playground falls compare with other causes of TBI?
The study does not compare playgrounds with other causes of TBIs in children. It does cite a 2011 CDC report [pdf link] on nonfatal TBIs related to sports and recreation among American children aged under 20 years, stating that this report “estimated that … playground activities accounted for the highest estimated number of ED visits among the activities examined.” This statement is incorrect: the CDC report cited shows playground activities third behind bicycling and football for children aged under 20 years (see Table 2 of the CDC paper). For children aged under 15 years the picture is not as clear, because the data presented is incomplete. However, it suggests that even for this age group, bicycling accounted for more ED visits than playgrounds (see Table 3 of the CDC paper).
Other studies suggest that overall, playground falls make up a small proportion of ED visits for TBIs, and that several other causes are more significant. For instance, this 2014 study on TBIs of children aged 3 – 18 in Ontario showed that playground equipment accounted for about 4 per cent of such visits, and were the 8th most common cause. Hockey/skating, motor vehicle accidents, football/rugby, snow sports, cycling, baseball and soccer all caused more ED visits than playground equipment.

What might explain the changes over time?
The paper offers a number of possible explanations for the rise in ED visits. These include: increased participation in playground activities; increased TBI incidence over time; and heightened public awareness of TBI and concussions. They point to four factors that could explain heightened awareness, including public education campaigns, media coverage of sports injuries, state laws on concussion and ‘return-to-play’, and the issue of TBI amongst returning military personnel from Iraq and Afghanistan. The authors do not offer further commentary on the changes: they do not discuss why playground participation might have risen since 2005, or why TBI incidences might have risen.
What are the authors’ conclusions?
The authors conclude that “strategies to reduce the incidence and severity of TBIs sustained on playgrounds are needed.” They state that strategies could “address design, surfacing, and maintenance.” They also point to “appropriate supervision and child behavior modification” as possible responses. The assumption is that existing TBI rates are too high, and the implication is that effective strategies are available to reduce them further. However, there is no discussion to support this assumption, and no evidence is given on the merits of different playground injury prevention strategies.
What does the study tell us about surfacing in playgrounds?
The study did not look at surfacing. Hence it cannot tell us anything about the effectiveness of different types of surfacing. The paper states that the NEISS-AIP data “do not provide detailed information about injury circumstances, such as playground surfacing and risk behaviors. As a result, NEISS-AIP cannot be used to assess the impact of these factors on injury incidence.”
Acknowledgements
Thanks to Brandy Tanenbaum at RBC First Office for Injury Prevention in Toronto for bringing to my attention the 2014 Ontario study on TBIs in children.


You open with: “… it is being seen by some as providing evidence for reviving the playground surfacing proposal that ASTM ultimately rejected last year.” and you close with: “… NEISS-AIP cannot be used to assess the impact of these factors on injury incidence” and in between is a superb forensic*analysis.
Bravo!
I mean your analysis of the claims, not their forensics! I suspect that even the disgraced South Yorkshire police would find their contentions problematic.
Its very gratifying to see you seize an emerging and increasingly important and contentious issue within your field of endeavour and push it hard in the public realm, challenging vested interests, sticking to your values and commitments to and on behalf of children, without fear (NoFear?) of opprobrium.
Again, bravo. I could say “you go, girl!” but that would be “inappropriate”. More power to your elbow. I’m not aware of anybody else who is taking up the knightly mantle and attempting to slay The Dragon Of Elfansafety.
Thanks for this fulsome praise Arthur. Others are taking up the issue, here in the UK (my sometime collaborators David Ball, Harry Harbottle and Bernard Spiegal for three), in North America (Dr Mariana Brussoni of the BC Injury Research and Prevention Unit for one) and in Australia (where Play Australia recently published an Aussie version of Managing Risk in Play Provision). In my view most or all of the members of the Play Safety Forum, while not in agreement on everything, have a shared concern about what might be called ‘mission creep’ in relation to equipment standards, especially around surfacing. But I’ll take due credit for my efforts to interpret and share the evidence.
Number crunching things that can be measured mostly, it sometimes seems, because they CAN be measured once again detracts from proportionality. Running these results through even the most basic Benefit – Risk analysis would reveal that the Benefits overwhelmingly outstrip the Risks. Moreover, researchers will always tend to focus on arguments that support the blatantly obvious: if you fall over it hurts.
Conversely, researchers will stay well clear of the difficult issues. In academic circles the maxim “publisher or die” is immensely influential. Research into something that does not produce a positive finding will never result in a published paper. Research, for example, into why some children become obese while others don’t. OK, there is stuff about eating, what, when, why and so forth, but what about obesity and exercise? We know it’s not as simple as ‘calories in (food) versus calories out (exercise) because the maths don’t work. But we intuitively know there is a link. So it must be more complex, more subtle, and perhaps more psychological than physiological. Self-esteem, the need for physicality, the sense of exploration, self-control. All things observed every day in the play-ground.
But where are the published papers?
All links gratefully received!
Marcus
Could it be childe are not getting enough risky play to help them develop appropriate body and safety awareness, therefore children have a more difficult time being safe?
Thanks for the comments – keep them coming. Marcus – you are right that measuring benefits (like learning or even physical activity) is harder than counting injuries and ED attendances. I’m sure you’ve come across the work on risky play by Ellen Sandseter. Do you know of the systematic literature review on the topic carried out by her and others, including Dr Mariana Brussoni (the BC injury prevention researcher)? Jill – you could have a point. It’s certainly plausible, though it would be hard (but not impossible) to back up with numbers.
Pingback: Gotta Love TV News: “Playground Fun Could Lead to Tragedy — Tune In at 10!” | Free Range Kids